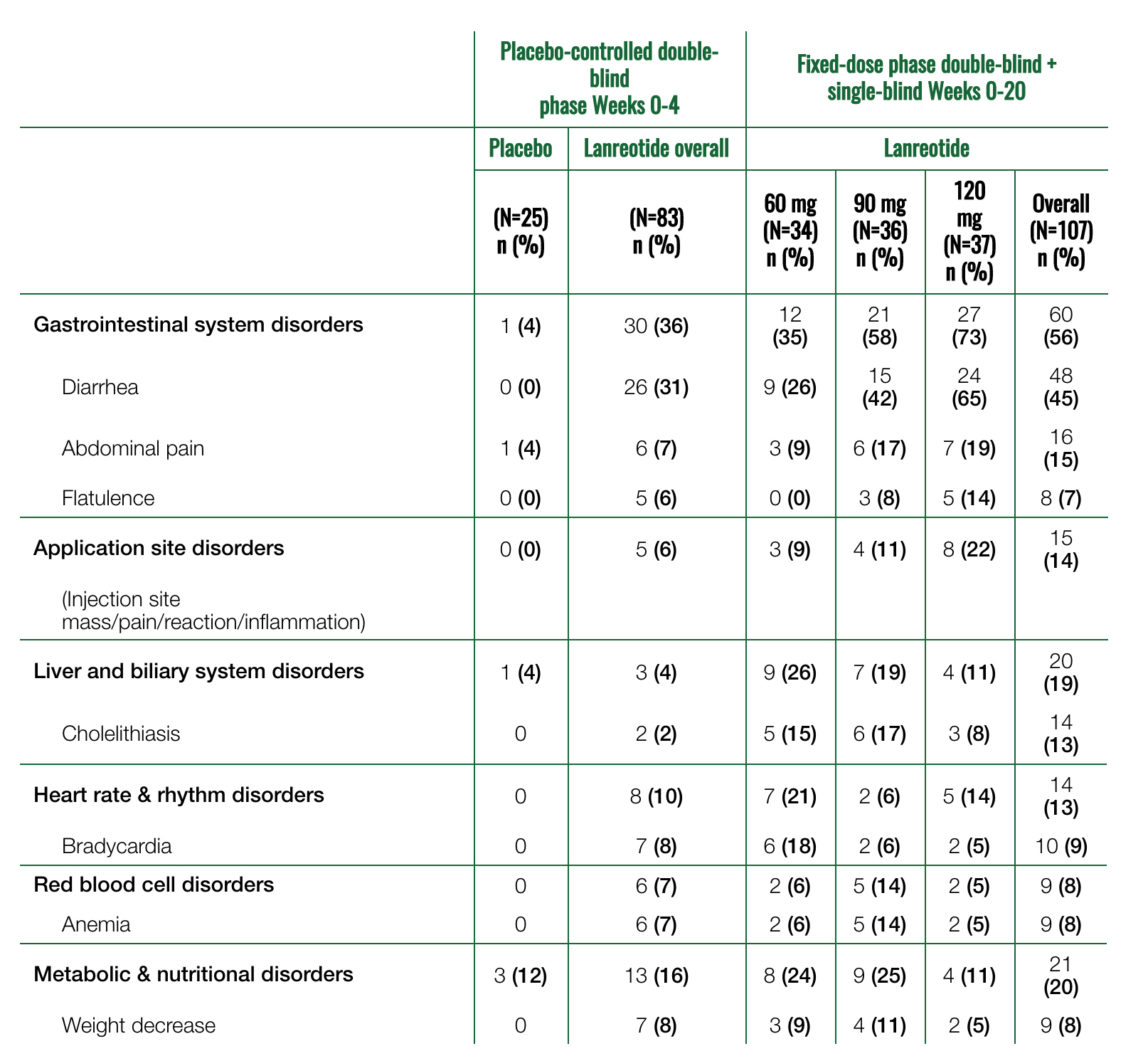
Most common adverse events occurring at an incidence >5% and at a higher rate than placebo in pivotal trial 11*
A patient is counted only once for each body symptom and preferred term.
Adverse reactions of dysglycemia (hypoglycemia, hyperglycemia, diabetes) were considered related to study drug in 7% (24/332) of patients1
In the pooled clinical studies (N=416), the majority of gastrointestinal reactions were mild to moderate in severity1
1% of acromegalic patients treated with Somatuline® Depot (lanreotide) Injection in the pooled clinical studies discontinued treatment because of gastrointestinal reactions1
*Data are from pivotal trial 1. Somatuline Depot was administered at 4-week intervals at doses of 60, 90, or 120 mg.
SOMATULINE DEPOT is contraindicated in patients with hypersensitivity to lanreotide. Allergic reactions (including angioedema and anaphylaxis) have been reported following administration of lanreotide.
Warnings and Precautions
Cholelithiasis and Gallbladder Sludge
SOMATULINE DEPOT may reduce gallbladder motility and lead to gallstone formation.
Periodic monitoring may be needed.
If complications of cholelithiasis are suspected, discontinue SOMATULINE DEPOT and treat appropriately.
Hypoglycemia or Hyperglycemia
Patients treated with SOMATULINE DEPOT may experience hypoglycemia or hyperglycemia.
Blood glucose levels should be monitored when SOMATULINE DEPOT treatment is initiated, or when the dose is altered, and antidiabetic treatment should be adjusted accordingly.
Cardiovascular Abnormalities
SOMATULINE DEPOT may decrease heart rate.
In cardiac studies with acromegalic patients, the most common cardiac adverse reactions were sinus bradycardia, bradycardia, and hypertension.
In patients without underlying cardiac disease, SOMATULINE DEPOT may lead to a decrease in heart rate without necessarily reaching the threshold of bradycardia.
In patients suffering from cardiac disorders prior to treatment, sinus bradycardia may occur. Care should be taken when initiating treatment in patients with bradycardia.
Thyroid Function Abnormalities
Slight decreases in thyroid function have been seen during treatment with lanreotide in acromegalic patients.
Thyroid function tests are recommended where clinically appropriate.
Monitoring/Laboratory Tests: In acromegaly, serum GH and IGF-1 levels are useful markers of the disease and effectiveness of treatment.
Steatorrhea and Malabsorption of Dietary Fats
New onset steatorrhea, stool discoloration and loose stools have been reported in patients receiving somatostatin analogs, including SOMATULINE DEPOT. Somatostatin analogs reversibly inhibit secretion of pancreatic enzymes and bile acids, which may result in malabsorption of dietary fats and subsequent symptoms of steatorrhea, loose stools, abdominal bloating, and weight loss.
If new occurrence or worsening of these symptoms are reported in patients receiving SOMATULINE DEPOT, evaluate patients for potential pancreatic exocrine insufficiency and manage accordingly.
Most Common Adverse Reactions
Adverse reactions in >5% of patients who received SOMATULINE DEPOT were diarrhea (37%), cholelithiasis (20%), abdominal pain (19%), nausea (11%) injection-site reactions (9%) constipation (8%) flatulence (7%) vomiting (7%) arthralgia (7%) headache (7%) and loose stools (6%).
Drug Interactions
SOMATULINE DEPOT may decrease the absorption of cyclosporine (dosage adjustment may be needed); increase the absorption of bromocriptine; and require dosage adjustment for bradycardia-inducing drugs (e.g., beta-blockers).
Special Populations
Lactation: Advise women not to breastfeed during treatment and for 6 months after the last dose.
Moderate to Severe Renal and Hepatic Impairment: See full prescribing information for dosage adjustment in patients with acromegaly.
SOMATULINE® DEPOT (lanreotide) is a somatostatin analog indicated for the long-term treatment of patients with acromegaly who have had an inadequate response to surgery and/or radiotherapy, or for whom surgery and/or radiotherapy is not an option. The goal of treatment in acromegaly is to reduce growth hormone (GH) and insulin growth factor-1 (IGF-1) levels to normal.
You are about to leave SomatulineDepot.com/HCP/Acromegaly. This link is provided as a service to our website visitors. It will take you to a website maintained by a third party who is solely responsible for its content.
Ipsen does not control, recommend, endorse or accept liability for sites controlled by third parties.
You are about to leave SomatulineDepot.com/HCP/Acromegaly. This link is provided as a service to our website visitors. It will take you to another website maintained by Ipsen.